
Exposure Assessment Tools by Routes - Inhalation
On this page:
Overview

An exposure routeThe way a chemical pollutant enters an organism after contact, e.g., by ingestion, inhalation, or dermal absorption. is the way that a contaminant enters an individual or population after contact (IPCS, 2004). Typically, exposure occurs by one of three exposure routes—inhalation, ingestion, or dermal.
Inhalation exposure can result from breathing air that is contaminated with particulate matter (e.g., dust), vapors (e.g., volatile or semivolatile contaminants), or aerosols. Individuals can be exposed via the inhalation route during a variety of activities outdoors and indoors. Indoor receptors could also be exposed to outdoor air contaminants that infiltrate the indoor environment.
Estimating exposure from inhalation requires information on the concentrations of contaminants in the air and the timeframe over which inhalation exposure occurs. To calculate an inhaled dose, inhalation rates and receptor body weights might also be needed.
Calculations to estimate dose from inhalation are provided in this module as are various tools available for evaluating potential exposure concentrations. Exposure scenarios, exposure factors, and guidance for assessing exposure via inhalation are also provided.
Methods
When a contaminant is taken into the body via inhalation, the amount that gets into the body in a biologically available form is called the doseThe amount of a substance available for interactions with metabolic processes or biologically significant receptors after crossing the outer boundary of an organism.. There are a few different ways to measure dose (U.S. EPA, 1992):
- Potential dose is the amount of contaminant inhaled (i.e., amount that gets in the mouth or nose), not all of which is actually absorbed.
- Applied dose is the amount of contaminant at the absorption barrier (e.g., respiratory tract) that can be absorbed by the body.
- Internal dose is the amount of contaminant that gets past the exchange boundary (lung) and into the blood, or the amount of the contaminant that can interact with organs and tissues to cause biological effects.
- Biologically effective dose is the amount of contaminant that interacts with the internal target tissue or organ.
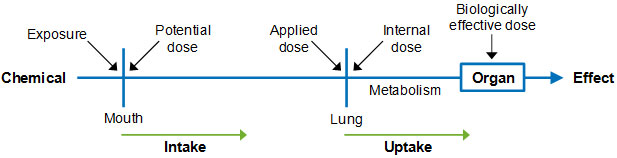
The amount of chemical that is absorbed through the lung may vary from the amount of the substance that is inhaled. Thus, internal dose might differ from potential dose.
When using inhalation reference concentrations [RfCs] or inhalation unit risk [IURs] from the Integrated Risk Information System (IRIS) to characterize risk, it is not necessary to calculate the inhaled dose. This is because the IRIS methodology accounts for inhalation rates in the development of “dose-response” relationships. Instead, only an air concentration is needed to evaluate health concerns.
The methods used in developing noncancer inhalation dose-response values for IRIS are discussed in more detail in the U.S. EPA report entitled Methods for Derivation of Inhalation Reference Concentrations and Application of Inhalation Dosimetry (U.S. EPA, 1994).
The Superfund Program has also recently updated its approach for determining inhalation risk. It has eliminated the use of inhalation rates when evaluating exposure to air contaminants. This is described in Risk Assessment Guidance for Superfund (Part F, Supplemental Guidance for Inhalation Risk Assessment) (U.S. EPA, 2009).
This updated methodology recommends that risk assessors use the concentration of the contaminant in air (Cair) as the exposure metric (e.g., mg/m3) instead of the intake of a contaminant in air based on inhalation rate and body weight (dose; e.g., mg/kg-day).
Calculations
Using EPA’s current methodology, it is unnecessary to calculate an inhaled dose when using dose-response factors from IRIS in a risk assessment. However, inhalation risk assessments may require that an adjusted air concentration be used to represent continuous exposure.
The adjusted air concentration (Cair-adj) may be estimated as shown below. As described under the Methods tab, for noncarcinogens, the air concentration is adjusted based on the time over which exposure occurs (i.e., the exposure duration). For carcinogens, the concentration is averaged over the lifetime of the exposed individual (often assumed to be 70 years).
Where:
Cair = Concentration of contaminant in air (mg/m3)
ET = Exposure time (hours/day)
EF = Exposure frequency (days/year)
ED = Exposure duration (years)
AT = Averaging time (days)
- The concentration in air (Cair) is either a measured or modeled value. Air concentrations may be measured in the breathing zone of individuals using personal monitoring equipment or in indoor or outdoor air using stationary or portable monitoring devices. Air measurements may represent gas phase or particulate-phase contaminants, or both.
- Temporal parameters in the equation include the following:
- Exposure time (ET) and exposure frequency (EF) refer to the frequency with which the exposure occurs and might be provided in hours per day and days per year, respectively.
- Exposure duration (ED) is the amount of time that an individual or population is exposed to the contaminant being evaluated and is typically given in years.
- Averaging time (AT) is the amount of time over which exposure is averaged and is equal to ED for assessing non-cancer risks. For chronic assessments (e.g., cancer), potential lifetime average daily dose (LADD) is calculated in which lifetime (LT, in days) is substituted for AT.
In some cases, it may be necessary to calculate an inhalation dose using the equation below. This algorithm can be used to calculate the average daily potential dose from inhalation of a contaminant in air.
The potential dose of a contaminant is the product of the contaminant concentration, inhalation rate, exposure time, exposure frequency, and exposure duration divided by the product of averaging time and body weight. The equation parameters below must be defined for each inhalation exposure scenario, and all parameters must be expressed in consistent units.
In some cases, unit conversion factors may be necessary. Average Daily Dose (ADD) is generally expressed as mass of contaminant per unit body weight over time (e.g., mg/kg-day).
Where:
ADD = Average daily dose (mg/kg-day)
Cair = Concentration of contaminant in air (mg/m3)
InhR = Inhalation rate (m3/hour)
ET = Exposure time (hours/day)
EF = Exposure frequency (days/year)
ED = Exposure duration (years)
BW = Body weight (kg)
AT = Averaging time (days)
See above for descriptions for many of the relevant equation parameters. The additional parameters are described below.
- Inhalation rate (InhR) represents the volume of air inhaled over a specified timeframe. Long-term inhalation rates are typically expressed in units of m3/day. Short-term inhalation rates are typically indexed to activity levels and are expressed in units of m3/hour or m3/minute. Assessors should choose inhalation rate data that best represent the population for which exposures are being assessed. Chapter 6 of the Handbook provides inhalation rate data for various age groups (see the Factors tab in this module).
- Body weight (BW) of an individual, typically expressed in kilograms (kg), is also included so that the dose is normalized to that value. Sometimes the inhalation rate is already normalized to body weight (e.g., in units of m3/kg-day). In this case, a separate term for body weight would not be necessary.
Additional information on exposure scenarios involving the inhalation route can be found in the Indirect Estimation Module in the Approaches Tool Set.
Concentrations
Sources of contamination to air, water, and soil and dust are discussed in the Media Tool Set. Media-specific concentrations are needed for estimating exposure via the inhalation route. Data and tools that can be used to estimate media-specific concentrations can also be found in the Media Tool Set.
Contamination of ambient (outdoor) air can occur from anthropogenic or natural sources. Examples of anthropogenic sources include: driving cars, trucks, or buses; burning coal, oil, and other fossil fuels; manufacturing chemicals or other products; degreasing, painting, or other industrial operations; and dry cleaning. Examples of natural sources include: gases emitted by the earth’s crust [e.g., radon], and smoke and carbon dioxide [CO2] released during forest fires.
Activities such as these may add gases and/or particles to the air. Some air pollutants can remain in the environment for long periods of time and can be transported in the atmosphere (e.g., by wind) hundreds of miles from their original source.
There are many sources of indoor air contaminants. These contaminants can enter buildings from the outside or may be generated from inside sources. Examples of indoor sources include: combustion of oil, gas, kerosene, coal, wood, and tobacco products; building materials and furnishings; and consumer products).
Reductions in building ventilation may increase indoor pollutant levels because indoor emissions are not being diluted by outdoor air or carried out of the indoor environment. Temperature and humidity can also contribute to increases in contaminant concentrations indoors.
Contaminant concentrations in air can be characterized based on measurements, modeling, and/or available monitoring data.
Measuring Concentrations
Information on sampling techniques and analytical methods is available to support the measurement of contaminants in potentially inhaled media.
Modeling Concentrations
In the absence of measurement data, a variety of models can be used to estimate contaminant concentrations in air or dust that may be inhaled. Ambient air quality models may be used to estimate contaminant concentrations in air considering spatial-temporal characteristics (e.g., urban versus rural, geographic scale; climate, season). Some models also account for population demographics and the time that the exposed populations spend in various microenvironments.
Indoor air models and models that evaluate air concentrations for specific exposure scenarios are also available. Examples include: inhalation of contaminants that volatilize from water while showering, and inhalation of contaminants that volatilize from pool water while swimming.
Available Data
Personal or stationary monitors can be used to measure air concentrations in the breathing zone of individuals who are closest to a source. Area monitors may be used to measure air concentrations that are representative of particular areas. In some cases, measurement data are used directly to estimate exposure concentrations. In other cases, measured data are used along with modeling to predict potential levels of exposure.
There are a number of information sources that provide monitoring data on contaminant concentrations in potentially inhaled media. Many of these data sources provide ambient air concentrations of contaminants at the national level and for other broad geographic areas such as cities, counties, and states. As such, they help EPA identify specific air toxics, and specific source sectors such as stationary sources or mobile sources, that generally produce the highest exposures and risks.
Scenarios
Inhalation exposure can be relevant for ambient air, indoor air, or both depending on the source and nature of the pollutant. Inhalation exposure can be estimated by first defining the exposure scenario of interest.
Exposure scenarios typically include information on the sources and pathways of exposure, contaminants of concern, and receptor populations. They might also describe a receptor population’s activities that may affect exposure and the timeframe over which exposure occurs.
Inhalation exposure could occur over short durations (e.g., more than 24 hours, up to 30 days) or longer timeframes (e.g., more than 30 days), and can be associated with various types of activities (e.g., occupational, recreational, residential) in different indoor or outdoor environments.
The table below provides some examples of inhalation scenarios. The list of examples is not meant to be exhaustive; there are numerous other inhalation scenarios that may be constructed based on the specific needs of the assessment. There are also numerous variations of the examples provided in the table.
| Medium | Receptor Population | Activity/Timeframe | Inhalation Rate | Exposure Period |
|---|---|---|---|---|
| Ambient air | General population; adults | Routine activity; long-term; adjusted air concentration | Not applicable | Chronic |
| Ambient air; contaminated site | School children | Playing during time spent in elementary school; dose calculation [Table 16-17] |
Short-tem, activity-specific [Table 6-2] |
Sub-chronic |
| Ambient air; source-related contaminant | Highly-exposed local population; adults and children | Routine; long-term-dose calculation | Daily [Table 6-1] |
Chronic or sub-chronic, depending on lifestage |
| Outdoor air; particulates from contaminated site | Occupational; adults | Site-specific construction; short-term; adjusted air concentration | Not applicable | Acute |
| Indoor air | Infants or home-bound elderly adults | Routine; less than lifetime; adjusted air concentration | Not applicable | Sub-chronic |
| Indoor air | Occupational | Working in contaminated office building; long-term occupational; adjusted air concentration [Table 16-8] |
Not applicable | Chronic |
| Indoor air; consumer product use | Consumers | Cleaning with same consumer product over long timeframe [Chapter 17] |
Short-term, activity-specific [Table 6-2] |
Chronic |
| Indoor air; vapor intrusion from under-foundation source | Residential adults and children | Routine over lifetime; adjusted air concentration | Not applicable | Chronic |
| Indoor air; volatilization from water while showering | Residential adults and children | Showering daily [Table 16-1] |
Short-term, activity-specific [Table 6-2] |
Chronic or sub-chronic, depending on lifestage |
| Outdoor or indoor air; volatilization from swimming pool water | Recreators | Swimming over less than lifetime [Table 16-1] |
Short-term, activity-specific [Table 6-2] |
Sub-chronic |
| Indoor air; contamination in vehicle | Commuters; adults | Traveling in vehicle to and from work; less than lifetime [Table 16-24] |
Short-term, activity-specific [Table 6-2] |
Sub-chronic |
Several resources are available that illustrate inhalation exposure scenarios.
Factors
MicroenvironmentsWell-defined surroundings such as the home, office, or kitchen that can be treated as uniform in terms of stressor concentration. are the various changing spaces in which people spend their time that will influence how they will be exposed to contaminants. A microenvironment can be defined as a space with a contaminant concentration that is assumed to be relatively well-mixed, homogeneous, and temporally constant while an individual is located within the microenvironment. Examples of microenvironments included in EPA assessments are automobiles, schools, work places, and other buildings. The Exposure Factors Handbook: 2011 Edition presents data on the amount of time that an individual is expected to spend in various microenvironments. For buildings, important factors might include size, volume, number of windows, and air exchange rates, and the Handbook provides information about these factors for both residential and nonresidential buildings (U.S. EPA, 2011).
To estimate human exposure to contaminants in ambient or indoor air, information is needed about the exposed population(s), exposure pathways, and the concentrations of contaminants in air. When determining inhalation risk, inhalation rate and body weight might not be needed. The Superfund Program’s updated approach for determining inhalation risk eliminates use of inhalation rates when evaluating exposure to air contaminants (U.S. EPA, 2009).
However, if inhalation rates are needed, data are available in Chapter 6 of the Handbook. Inhalation rate is a volume of air inhaled per unit time. Long-term inhalation rates are reported as daily rates in units of m3/day or m3/kg-day. Short-term rates are described for various activities (e.g., walking, running, playing, housework, yard work) or activity levels (e.g., light, moderate, heavy) in units of m3/minute.
Characteristics of the exposed individual and population are important to define because they determine inhalation rate. For example, inhalation rates will vary between children and adults due to differences in size, physiology, behavior, and activity levels. Individuals in an occupational setting are often assumed to be working harder than residents and so might be assumed to have a higher inhalation rate.
Personal characteristics also dictate activity patterns, which determine where a person is located (i.e., his/her microenvironments; see text box). They also pertain to the intensity of the activities in which the individual is engaged.
The Exposure Factors Tab of the Indirect Estimation Module provides links to data on inhalation rates.
Activity-specific factors that may be relevant for assessing inhalation exposures associated with specific activity levels are available in Chapter 16 of the Handbook. Other exposure factors that might be needed for assessing inhalation exposures include:
Other exposure factors that might be needed for assessing inhalation exposures include:
- Body weight (Chapter 8)
- Consumer product use (Chapter 17)
- Life expectancy values, specifically when evaluating cancer risk (Chapter 18)
- Building characteristics when assessing indoor air exposures (Chapter 19)
Inhalation exposure factors should be selected to represent the age, sex (if appropriate), timeframe/activity level, and population group (e.g., resident, occupational worker) for the exposure scenario of interest.
The Exposure Factors Tab of the Indirect Estimation Module provides links to data on other factors.
Guidance
The following sources provide helpful information for conducting exposure assessments involving the inhalation route of exposure.
References
- IPCS (International Programme on Chemical Safety). (2004). IPCS Risk Assessment Terminology: Part 2: IPCS Glossary of Key Exposure Assessment Terminology (PDF) (122 pp, 951 K, About PDF) . Geneva, Switzerland: World Health Organization.
- U.S. EPA. (1992). Guidelines for Exposure Assessment. (EPA/600/Z-92/001). Washington, DC.
- U.S. EPA. (1994). Methods for Derivation of Inhalation Reference Concentrations (RfCs) and Application of Inhalation Dosimetry. (EPA/600/8-90/066F). Washington, DC.
- U.S. EPA. (2009). Risk Assessment Guidance for Superfund (RAGS), Volume I: Human Health Evaluation Manual (Part F, Supplemental Guidance for Inhalation Risk Assessment): Final. (EPA/540/-R-070/002). Washington, DC.
- U.S. EPA. (2011). Exposure Factors Handbook 2011 Edition (Final). (EPA/600/R-09/052F). Washington, DC.